Paper:
Cross-Sectional Study of the Association Between Housing Type Post-Great East Japan Earthquake and Liver Enzymes: Tohoku Medical Megabank Community-Based Cohort Study
Shigeru Aiba*1,*2
 , Naoki Nakaya*1,*3, Mana Kogure*1,*3, Rieko Hatanaka*1,*3, Ippei Chiba*1,*3, Kumi Nakaya*1,*3, Masato Takase*1,*3, Sayuri Tokioka*1,*3, Tomohiro Nakamura*3,*4, Satoshi Nagaie*1,*3, Soichi Ogishima*1,*3, Yoko Izumi*1,*3, Nobuo Fuse*1,*3, Shinichi Kuriyama*1,*3,*5, and Atsushi Hozawa*1,*3,†
, Naoki Nakaya*1,*3, Mana Kogure*1,*3, Rieko Hatanaka*1,*3, Ippei Chiba*1,*3, Kumi Nakaya*1,*3, Masato Takase*1,*3, Sayuri Tokioka*1,*3, Tomohiro Nakamura*3,*4, Satoshi Nagaie*1,*3, Soichi Ogishima*1,*3, Yoko Izumi*1,*3, Nobuo Fuse*1,*3, Shinichi Kuriyama*1,*3,*5, and Atsushi Hozawa*1,*3,†
*1Graduate School of Medicine, Tohoku University
2-1 Seiryo-machi, Aoba-ku, Sendai, Miyagi 980-8573, Japan
*2Faculty of Nursing, Iryo Sosei University
Iwaki, Japan
*3Tohoku Medical Megabank Organization, Tohoku University
Sendai, Japan
*4Faculty of Data Science, Kyoto Women’s University
Kyoto, Japan
*5International Research Institute of Disaster Science, Tohoku University
Sendai, Japan
†Corresponding author

The Great East Japan Earthquake significantly impacted Japanese residents’ lives and housing conditions. Housing type after a disaster may affect liver function; however, few studies have reported this association. This study analyzed the association between housing type after the Great East Japan Earthquake and abnormal liver enzymes. This cross-sectional study included 35,531 participants (aged 40–74 years) from Miyagi Prefecture. Abnormal liver enzymes were defined as aspartate aminotransferase ≥40 IU/L or alanine aminotransferase ≥40 IU/L, or gamma-glutamyl transpeptidase ≥50 IU/L. To assess associations between housing type after the Great East Japan Earthquake and abnormal liver enzymes, prevalence odds ratios and 95% confidence intervals were calculated, adjusting for lifestyle variables, body mass index, and history of type 2 diabetes mellitus. Abnormal liver enzyme levels were observed in 19.2% of the participants. The adjusted prevalence odds ratios (95% confidence intervals) for abnormal liver enzymes among individuals who had lived in the same housing with half damage or more as before the Great East Japan Earthquake were 1.14 (1.04–1.26) compared with the reference group with less than half damage. High gamma-glutamyl transpeptidase levels contributed to the association between housing type after the Great East Japan Earthquake and individual liver enzyme levels. However, when stratified by sex and drinking status, these trends were not statistically significant. This study shows a significant association between maintaining the same housing as before the Great East Japan Earthquake and abnormal liver enzyme levels. Housing type can be considered in addressing liver dysfunction among disaster-affected residents.
1. Introduction
The Great East Japan Earthquake (GEJE) of March 11, 2011, caused extensive damage, resulting in 15,899 deaths and the collapse of 122,000 houses by March 10, 2021 1. Three years after the GEJE, several residents continued to experience significant lifestyle changes 2. Previous studies have reported a post-disaster increase in alcohol consumption 3,4 and the prevalence of hypertension and diabetes 5. Following the GEJE, an increase in body weight was observed among residents of prefabricated temporary housing 6,7, and a higher prevalence of diabetes was observed in evacuees from the nuclear power plant accidents 8. These findings suggest that the impact on lifestyle differs based on the housing type after the disaster.
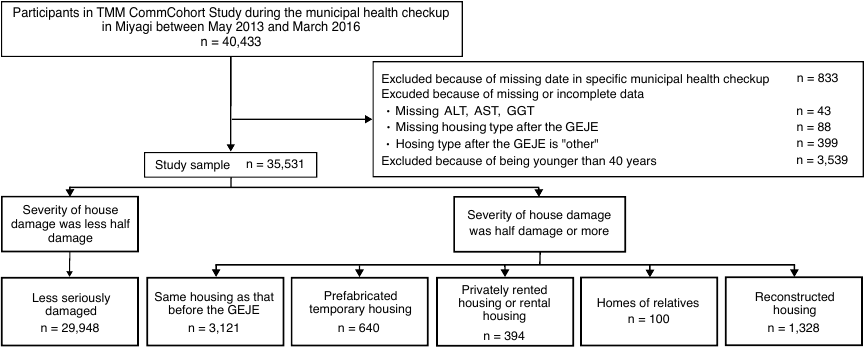
Fig. 1. Participant selection flowchart.
These lifestyle changes may lead to liver dysfunction. A retrospective cohort study of 569 Miyagi Prefecture residents (mean age 71.5 years) found increased gamma-glutamyl transpeptidase (GGT) levels post-GEJE among individuals in prefabricated temporary housing compared with those in pre-GEJE housing 9. Additionally, in a retrospective cohort study (\(n = 26{,}006\), mean age 67.8 years) of residents in Fukushima Prefecture, the prevalence of liver dysfunction was higher among evacuees than among non-evacuees following the GEJE and subsequent Fukushima Daiichi Nuclear Power Plant accident 10. Cirrhosis, an advanced stage of liver dysfunction, is caused by preventable factors in 90% of cases. However, three-quarters of patients are diagnosed at a late stage, when lifestyle modifications, such as weight loss and abstinence from alcohol, and etiological treatments, such as antiviral therapy, diminish their effectiveness 11. Representative indicators of liver dysfunction include blood tests for aspartate aminotransferase (AST), alanine aminotransferase (ALT), and GGT, which are also included in municipal health checkups. Therefore, a preventive approach, such as promptly encouraging medical consultation, is crucial when abnormalities in these indices are detected.
Previous studies showed that factors associated with elevated liver enzyme levels include being male 10, high alcohol consumption 12, obesity 12, visceral fat accumulation 13,14, and type 2 diabetes mellitus (T2DM) 15,16. Among these factors, obesity and T2DM are associated with mental distress 17,18, sleep duration 19,20, and inactivity 21,22, which could be related to housing type after the disaster 23,24,25. Prefabricated temporary housing is associated with economic insecurity and a high prevalence of individuals living alone 25. Conversely, privately rented or rental housing is associated with low physical activity and social capital levels 23. However, few studies have explored these effects and examined the link between different housing types and liver enzyme levels post-disaster 9,10. Similarly, few studies have fully investigated the impact of these effects on individuals who sustained damage to their housing without relocating post-GEJE.
In this study, we elucidated the association between housing type and high aspartate aminotransferase (AST), alanine aminotransferase (ALT), and GGT levels after the GEJE. We hypothesized that housing types after the disaster were associated with high liver enzyme levels, potentially related to drinking status, obesity, and T2DM. We analyzed data from a cohort study of approximately 35,000 residents in the Tohoku University Tohoku Medical Megabank (TMM) Organization.
2. Materials and Methods
2.1. Study Design and Participants
The TMM CommCohort Study 26 is a community-based prospective cohort study conducted in 2013 in Miyagi and Iwate Prefectures in coastal areas severely affected by the GEJE. Inclusion criteria included individuals aged \(\ge 20\) years who were registered in the basic resident register of all municipalities in Miyagi and Iwate Prefectures at the time of enrollment. Recruitment was performed using two major approaches: the Type 1 survey was performed at specific municipal health check-up sites, and the Type 2 survey was performed in an assessment center, the Community Support Center in Tohoku University Tohoku Medical Megabank Organization, and the Satellite at Iwate Medical University Iwate Tohoku Medical Megabank Organization. In the Type 1 survey, the age of the study participants ranged from 20 to 74 years. This study included 40,433 Type 1 survey participants who lived in Miyagi Prefecture and were recruited between May 2013 and March 2016.
Overall, 4,902 participants were excluded owing to missing data from specific municipal health check-up sites (\(n = 833\)), missing data on AST, ALT, and GGT (\(n = 43\)), incomplete responses or “other” regarding post-GEJE housing type in self-reported questionnaires (\(n = 487\)), or being younger than 40 years in comparison with previous studies 9,10 (\(n = 3{,}539\)) (Fig. 1). Overall, 35,531 individuals were included in the analysis.
2.2. Housing Type After the GEJE (Exposures)
Housing type following the GEJE, as reported during the survey, was considered the exposure variable. We employed a self-administered questionnaire to obtain information on home damage and housing type between May 2013 and March 2016 (2–5 years after the GEJE).
Home damage severity was categorized into “completely damaged (including all outflows),” “seriously damaged,” “half-damaged,” “partially damaged,” “no damage,” or “non-residence.” We categorized “partially damaged,” “no damage,” or “non-residence” into a unified reference group 27: “less than half damage.” Individuals reporting “completely damaged (including all outflows),” “seriously damaged,” or “half-damaged” were further classified as “same housing as that before the GEJE,” “prefabricated temporary housing,” “privately rented housing or rental housing,” “homes of relatives,” and “reconstructed housing” based on housing type at the time of survey 9,23. “The same housing as before the GEJE” was defined as a house in which they continued to live, although it was half or more damaged by the GEJE.
2.3. High Liver Enzymes (Outcomes)
AST, ALT, and GGT levels were assessed during the municipal health checkups between May 2013 and March 2016. Serum was extracted from 2 mL of the 34 mL blood sample and measured using the Japanese Society of Clinical Chemistry transferable method 26. Using reference criteria from a previous study 10, high levels of AST, ALT, and GGT were defined as \(\ge 40\) IU/L, \(\ge 40\) IU/L, and \(\ge 50\) IU/L, respectively. The primary outcome was abnormal liver enzyme levels, defined as AST \(\ge 40\) IU/L or ALT \(\ge 40\) IU/L or GGT \(\ge 50\) IU/L. The secondary outcomes were high AST, ALT, and GGT levels.
2.4. Covariates
Demographic and anthropometric characteristics, including sex, age, and body mass index (BMI), were extracted from municipal health checkups. Sociodemographic and health-related data were collected via self-administered questionnaires.
Psychological distress was assessed using the Kessler Psychological Distress Scale (K6) 28. Sleep conditions were evaluated using the Athens Insomnia Scale (AIS) 29. Drinking status was determined by calculating total ethanol intake, which was obtained by multiplying the frequency of alcohol consumption by the quantity consumed. Alcohol consumption was classified into six categories: sake, distilled spirits, shochu-based beverages, beer, whiskey, and wine. Alcohol intake frequency was classified into six categories: almost never, 1–3 days/month, 1–2 days/week, 3–4 days/week, 5–6 days/week, and daily. The participants indicated the quantity and alcohol type consumed. Physical activity was defined as the sum of the frequency of each physical activity for which the participants reported the average frequency [times/week] and duration [min/time] of the following four categories: normal walking, brisk walking, moderate-intensity exercise, and hard-intensity exercise. Snacking behavior was assessed as the sum of the average frequency [times/month, times/week, or times/day] of the following six categories: Japanese sweets, cakes, biscuits/cookies, chocolate, soft drinks, and energy drinks using the food frequency questionnaire.
Table 1. Characteristics of the study participants based on post-GEJE housing type.

2.5. Statistical Methods
The study participants were categorized into six groups based on post-GEJE housing type: “less seriously damaged (reference),” “same housing as that before the GEJE,” “prefabricated temporary housing,” “privately rented housing or rental housing,” “homes of relatives,” and “reconstructed housing.” Continuous variables are described as median, first quartile, and third quartile, whereas discrete variables are described as frequencies and proportions. Details on covariates are provided in Appendix A.
Second, multivariable logistic regression models were employed to investigate the association between housing type and high liver enzyme levels after the GEJE. This analysis yielded the crude prevalence odds ratios (PORs), adjusted PORs, corresponding 95% confidence intervals (CIs), and associated \(p\)-values. The less severely damaged group was used as the reference group. Three models were constructed to account for potential confounding factors. Model 1 controlled for age and sex. Model 2 additionally included the number of people in the household, educational background, smoking status, psychological distress, sleeping condition, physical activity, snacking behavior, and history of cardiovascular disease, building upon the covariates in Model 1. Model 3 further incorporated drinking status, BMI, and history of T2DM in addition to the factors in Model 2. In the multivariable logistic regression analyses, missing data for any covariates were classified into the “missing” category. PORs, their corresponding 95% CIs, and \(p\)-values were subsequently calculated using multivariable logistic regression models.
To assess the modification effect of sex and drinking status on liver enzymes, the analysis was performed according to sex or drinking status. To analyze drinking status, the study population was stratified into a group of non-drinkers and another combining light drinkers and drinkers to ensure adequate power for the analysis. Furthermore, to assess the impact of prior fatty liver diagnosis, respondents with a history of fatty liver (\(n = \textrm{1,427}\)) were excluded.
As a supplementary analysis, we performed logistic regression analysis using only the “no damage” category to confirm the validity of this reference group. Additionally, we performed a robust Poisson regression analysis to compensate for the overestimation of abnormal liver enzyme levels. Furthermore, we also performed the same multiple logistic regression analysis on individuals aged \(<40\) years, who were not included in the study and were at a low risk of having abnormal liver enzyme levels.
Statistical significance was set at \(p < 0.05\). Analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Table 2. PORs, 95% CIs and \(p\)-values between post-GEJE housing type and abnormal liver enzymes.

3. Results
Table 1 and Supplementary Table 6 in Appendix B present the characteristics of the study participants stratified by post-GEJE housing type. Individuals residing in prefabricated temporary housing, privately rented housing, or rental housing had a higher probability of living alone, having lower education, smoking, experiencing greater psychological distress, experiencing poorer sleep quality, reporting lower alcohol consumption, engaging in irregular physical activity, and being obese than those residing in pre-GEJE housing. This tendency did not change when participants with a history of fatty liver were excluded (Supplementary Table 7 in Appendix B). Table 2 and Supplementary Table 8 in Appendix B display the PORs, adjusted PORs (aPORs), and 95% CIs for abnormal liver enzyme levels, that is, high ALT, AST, and GGT levels based on post-GEJE housing, using “less than half damage” as the reference group. For abnormal liver enzyme levels, a significant difference was observed in all models, in those with the same housing as that before the GEJE (aPORs [95% CI]; 1.14 [1.04–1.26] in Model 3). Among individual liver enzyme values, only high GGT levels were statistically significant among individuals living in the same housing as before the GEJE. In prefabricated temporary housing, the aPORs (95% CIs) were 1.26 (1.03–1.53) in Model 2. The association was no longer statistically significant in Model 3, with the aPOR of 1.16 (0.95–1.42). There was no association between privately rented/rental housing and abnormal liver enzyme levels; however, a significant association was observed with high ALT levels. Similar trends were observed when the reference category was set to “no damage” (Supplementary Table 9 in Appendix B), and in the risk ratios for abnormal liver enzyme levels (Supplementary Table 10 in Appendix B). Given that adjusting for drinking status, BMI, and T2DM attenuated the relationships, we checked the relationship between covariates and abnormal liver enzyme levels and identified a significant relationship between drinking status and BMI (Supplementary Table 11 in Appendix B).
The sex-stratified analyses are presented in Table 3 and Supplementary Table 12 in Appendix B. This tendency did not differ between males and females.
Similarly, stratified analyses were performed according to drinking status (Table 4 and Supplementary Table 13 in Appendix B). A significant association between having the same housing as that before the GEJE and abnormal liver enzyme levels and high GGT levels was observed among drinkers, but not among non-drinkers. For the other housing types, the association with abnormal liver enzymes did not differ substantially between non-drinkers and drinkers.
After excluding participants with a self-reported history of fatty liver, the results showed similar overall trends (Table 5 and Supplementary Table 14 in Appendix B).
A supplementary analysis did not reveal a significant association between post-GEJE housing type and abnormal liver enzyme levels in individuals aged \(<40\) years (Supplementary Tables 15 and 16 in Appendix B).
Table 3. PORs, 95% CIs and \(p\)-values between post-GEJE housing type and abnormal liver enzymes stratified based on sex.

Table 4. PORs, 95% CIs and \(p\)-values between post-GEJE housing type and abnormal liver enzymes stratified based on drinking status.

Table 5. PORs, 95% CIs and \(p\)-values between post-GEJE housing type and abnormal liver enzymes without history of fatty liver.

4. Discussion
This cross-sectional study investigated the association between housing type and abnormal liver enzyme levels in 35,531 participants in Miyagi Prefecture after the GEJE. It was revealed that abnormal liver enzyme levels were more prevalent among individuals living in the same conditions as before the GEJE, particularly after their houses were completely, severely damaged or half damaged (compared with when they were less than half damaged). These associations were observed after adjusting for sex, age, lifestyle, BMI, and medical history. The same association was observed among individuals living in the same conditions as before the GEJE, particularly after their houses were completely, severely damaged or half damaged (compared with that observed in the light-drinker and drinker groups in the stratified analysis by drinking status).
Previous studies have revealed a link between post-GEJE housing and elevated liver enzyme levels. Increased GGT levels were observed among individuals in privately rented or rental housing post-GEJE compared with pre-GEJE 9. Additionally, evacuees showed a higher prevalence of liver dysfunction compared to non-evacuees following the GEJE and the subsequent Fukushima Daiichi Nuclear Power Plant accidents 10. The present findings are consistent with those of prior reports. Furthermore, these results demonstrate that high liver enzyme levels differed based on post-GEJE housing type.
4.1. Housing Type and Abnormal Liver Enzymes (Main Outcome)
In this study, a significant association between housing type and abnormal liver enzyme levels was observed in the full model for individuals residing in the same housing as before the GEJE, and this significant association persisted up to Model 2 for those living in prefabricated temporary housing. Because adjusting for drinking status, BMI, and T2DM attenuated the relationship between housing and abnormal enzyme levels, we confirmed the risk of covariates. Consequently, higher BMI and drinking status showed stronger associations with abnormal liver enzyme levels. Owing to the fact that 1) participants who lived in the same housing as before the GEJE included a larger proportion of drinkers and 2) individuals living in prefabricated housing exhibited higher BMI; therefore, we considered that drinking status and BMI might mediate the relationship between housing type (following the GEJE) and abnormal liver enzyme levels. Previous studies have reported an increase in alcohol consumption 3,4 and BMI 6,7,8 before and after a disaster. This study also suggests that similar changes may have occurred in the same housing as before the GEJE and in prefabricated temporary housing. Therefore, further studies, including longitudinal studies, are required.
When we stratified based on sex or history of fatty liver, the observed findings remained unchanged; however, some associations became statistically non-significant. This may have been due to the reduced statistical power caused by the smaller sample size. Therefore, no clear evidence was found to suggest that sex or self-reported history of fatty liver affected the relationship between housing condition and abnormal liver enzyme levels.
When examining the relationship by drinking status, the risk was higher for non-drinkers in prefabricated temporary housing, although this was not significant. Conversely, for light drinkers and drinkers, as with the overall results, a significant association was observed even after adjustment for the same housing as that before the GEJE, and a non-significant increase in risk was observed among individuals living in prefabricated temporary housing. The results for prefabricated temporary housing and liver function showed a similar trend to that of a previous study 10, which found that evacuation was associated with liver dysfunction even when stratified by drinking status. Contrarily, for the same housing as that before the GEJE, no association was found among non-drinkers, suggesting that the impact of drinking status and housing status on liver dysfunction may differ.
In this study, “same housing as that before the GEJE” refers to individuals living in their original damaged houses, a group often used as a reference in prior studies 9,23,25 and not typically considered at high risk. This study is important because it shows that careful observation is also necessary for people who remained in houses that were heavily damaged by the earthquake. Notably, the number of drinkers and people with BMI \(\ge 25\) kg/m\(^2\), related to abnormal liver enzyme levels, was high, and the characteristics of those who were less seriously damaged were different.
Although the number of subjects was limited, the absence of a significant association in analyses restricted to those under 40 years old (Supplementary Table 16 in Appendix B) suggests a potentially higher risk of abnormal liver enzymes among individuals over 40 years residing in the same pre-GEJE housing or prefabricated temporary housing after experiencing severe disaster-related damage. Therefore, a population-based approach could be adopted for the public, such as raising awareness through informational materials about the potential for deteriorating liver function indicators in those who have been seriously affected by a disaster. Furthermore, the town/city administration is reported to be the primary support providers relied upon by disaster victims 30, and policymakers can consider implementing a system where professionals conducting outreach for disaster victims are informed about the possibility of poor liver function indicators in residents of the same pre-GEJE housing and prefabricated temporary housing and are equipped to collect information on related lifestyle habits. While a previous study 27 utilized the actual degree of house damage as an exposure in examining its relationship with all-cause mortality, focusing on easily identifiable factors like housing type in this study is valuable for practical support efforts. However, the mechanisms underlying the relationship between housing type and liver function indicators require further investigation in future research.
4.2. Housing Type and Liver Enzymes (Secondary Outcome)
High ALT levels showed a significant association with living in privately rented or rental housing, and high GGT levels were observed in those living in the same housing as before the GEJE, even after adjusting for lifestyle variables. However, high AST levels were not significant predictors.
AST and ALT are markers of cellular and organ damage, respectively; ALT is particularly specific to the liver. Elevated AST and ALT levels are correlated with liver dysfunction 31. GGT level is an indicator of liver dysfunction and is particularly prone to elevation due to alcohol consumption 31. Although a previous study reported elevated GGT levels among privately rented or rental housing residents, this study found no significant positive correlation with high GGT levels. Only high ALT levels showed a significant positive correlation. Possible reasons for this include the higher proportion of women in the study population (60.1% in this study vs. 53.8% in the previous study), younger age group (median age of 64 years in this study vs. mean age of 71.5 years in the previous study), and a lower proportion of individuals with a BMI of at least 25.0 (30.4% in this study vs. 36.0% in the previous study) 9. These factors may have reduced the risk factors for elevated GGT levels; however, further detailed investigations are necessary.
Elevated GGT levels are positively associated with all-cause mortality 32,33,34,35. Individuals who continue to live as they did before the GEJE and those in prefabricated temporary housing with high GGT levels could face more health issues in the future. Furthermore, ALT levels at the upper limit of normal were associated with a high standardized mortality ratio 36 and with increased liver-related mortality 32. In the long term, high ALT levels in individuals residing in privately rented or rental housing could increase the risk of reduced life expectancy.
4.3. Limitations
The current study has five limitations. First, the cross-sectional design precluded the demonstration of a causal relationship. However, reverse causality was unlikely, as individuals with high liver enzyme levels were assigned to specific housing groups. Furthermore, although it was conditional during self-reporting, the exclusion of participants with a history of fatty liver disease did not alter the findings. We plan to conduct a longitudinal study to investigate the causal relationship between housing type and liver dysfunction. Second, the study population comprised individuals who joined the TMM CommCohort Study during municipal health check-ups and may have had a heightened interest in health. This factor could have introduced selection bias in the comparison and exposure groups. Consequently, the prevalence of high liver enzyme levels may have been underestimated in each group. Nonetheless, this limitation is not expected to significantly affect the relationship between post-GEJE housing type and high liver enzyme levels. In the Type 1 survey, 69.1% of individuals who underwent specific municipal health checkups participated in the TMM CommCohort Study 26, supporting the representativeness of the sample. Third, the housing types were misclassified after the GEJE. The study period was from May 2013 to March 2016, coinciding with a decrease in the number of residents in prefabricated temporary housing and privately rented housing to less than half in Miyagi Prefecture 37,38. Therefore, the observed association between high liver enzyme levels and prefabricated temporary, privately rented, or rental housing may have been underestimated. It is possible that this may also be a bias in the longitudinal study planned. Fourth, the size and number of events were relatively small for employing models with various explanatory and adjustment variables, potentially causing underpowered detection in some categories. Fifth, there is still the possibility of unmeasured confounding and the influence of residual confounding. Life events that occurred between 2011, the year of the earthquake, and 2013, the year of the survey, may have affected housing type after the disaster and poor liver function indicators. Other possible factors include changes in the living environment of the participants themselves and those around them, changes in the participants’ own eating, exercise, and drinking habits, and the influence of past and present medical histories that could not be collected through self-reporting.
In conclusion, this study revealed an association between post-GEJE housing type and abnormal liver enzyme levels, even after controlling for lifestyle variables, such as alcohol consumption, psychological distress, sleeping conditions, physical activity, snacking behavior, and medical history, which have not been adequately controlled for in previous studies. Housing type is an easily identifiable factor for identifying people needing assistance after a disaster. This study highlights that there are residents at high risk of liver dysfunction in disaster-affected areas, depending on their housing type.
Conflict of Interest: The authors declare none.
Authors’ Contributions: Conceptualization, S.A. and N.N. and M.K. and A.H.; methodology, A.S. and N.N. and M.K. and A.H.; formal analysis, S.A.; data curation, M.K.; writing-original draft preparation, S.A. and N.N. and M.K. and R.H. and I.C. and K.N. and M.T. and S.T. and T.N. and S.N. and O.S. and Y.I. and N.F. and S.K. and A.H.; supervision, N.N. and M.K. and A.H.; project administration, A.H.; funding acquisition, A.H. All authors have read and agreed to the published version of the manuscript.
IRB Approval Code and Name of the Institution: Written informed consent was obtained from each participant, and those who did not provide consent were excluded. The Institutional Review Board of the Tohoku Medical Megabank Organization approved this study (approval numbers 2012-4-617 [initial approval] and 2021-4-113 [latest approval]).
Data availability: All data used to support the findings of this study may be released upon application to the Tohoku Medical Megabank Organization (Sendai, Japan), which can be contacted by Professor Atsushi Hozawa (hozawa@megabank.tohoku.ac.jp).
Appendix A. Details on Covariates
The covariates were categorized as follows: Sex was classified as male or female. Age was divided into four categories at the time of the survey: 40–49, 50–59, 60–69, and 70–74 years. The number of household members was classified into 1 or \(\ge 2\). Educational background was classified into four categories: elementary / junior high / high school, professional training college / junior college / college of technology, university / graduate school, and others. Smoking status was classified into three categories: never smoked, ex-smoker, and current smoker. Participants who had smoked fewer than 100 cigarettes in their lifetime were categorized as never smoked, more than 100 cigarettes but were not currently smoking as ex-smokers, and those who had more than 100 cigarettes and were currently smoking as current smokers. Psychological distress was classified into \(\textrm{K6} <10\) or \(\textrm{K6} \ge10\) 9,24. Sleep condition was classified into \(\textrm{AIS} < 6\) or \(\textrm{AIS} \ge 6\) 9,22. Physical activity was classified as habitual or non-habitual. Participants were classified as habitual if they engaged in activities \(\ge 2\)/week for 30 min; others were defined as non-habitual. Snacking behavior was classified as habitual if participants consumed sweets or drinks \(\ge\) 1/day; otherwise, they were defined as nonhabitual. History of cardiovascular disease was classified as “yes” or “no.” Participants with a history of cerebral hemorrhage, cerebral infarction, subarachnoid hemorrhage, or myocardial infarction/angina pectoris were defined as “yes.” Others were defined as “no.” Drinking status was classified into four categories: non-drinker, ex-drinker, light drinker, and drinker. Participants with alcohol intake of \(<23\) g/day were classified as light drinkers. Participants with alcohol intake of \(\ge 23\) g/day were classified as drinkers. BMI was stratified into \(<18.5\), 18.5 to \(<25\), and \(\ge 25\) kg/m\(^2\). The history of T2DM was classified as “yes” or “no.” Participants with a history of T2DM were defined as “yes,” whereas others were defined as “no.”
Appendix B. Supplementary Tables
This appendix contains Supplementary Tables 6–16.
Table 6. Characteristics of the study participants based on post-GEJE housing type (homes of relatives, reconstructed housing).

Table 7. Characteristics of the study participants based on post-GEJE housing type without history of fatty liver.

Table 8. PORs, 95% CIs and \(p\)-values between post-GEJE housing type (homes of relatives, reconstructed housing) and abnormal liver enzymes.

Table 9. PORs, 95% CIs and \(p\)-values between post-GEJE housing type (refer to “no damage”) and abnormal liver enzymes.

Table 10. RRs, 95% CIs and \(p\)-values between post-GEJE housing type and abnormal liver enzymes by a robust Poisson regression analysis.

Table 11. PORs and 95% CIs for each adjusted variable in Model 3 of logistic regression analysis on abnormal liver enzymes.

Table 12. PORs, 95% CIs, and \(p\)-values between post-GEJE housing type (homes of relatives, reconstructed housing) and abnormal liver enzymes based on sex.

Table 13. PORs, 95% CIs, and \(p\)-values between post-GEJE housing type (homes of relatives, reconstructed housing) and abnormal liver enzymes based on drinking status.

Table 14. PORs, 95% CIs, and \(p\)-values between post-GEJE housing type (homes of relatives, reconstructed housing) and abnormal liver enzymes without history of fatty liver.

Table 15. Characteristics of the study participants based on post-GEJE housing type \(<40\) years.

Table 16. ORs, aORs, 95% CIs, and \(p\)-values between post-GEJE housing type and abnormal liver enzymes \(<40\) years.

Acknowledgments
The authors sincerely express their gratitude to the people of Japan and the world for their valuable support in the Great East Japan Earthquake-affected areas after the disaster. We thank all participants and municipal staff who helped with our project. We also thank the members of the Tohoku Medical Megabank Organization and Iwate Tohoku Medical Megabank Organization, including the Genome Medical Research Coordinators, office and administrative personnel, and software engineers, for their assistance with the projects. The complete list of members is available at https://www.megabank.tohoku.ac.jp/english/a230901/ for the Tohoku Medical Megabank Organization and at http://iwate-megabank.org/en/about/departments/ for the Iwate Tohoku Medical Megabank Organization. This work was supported in part by the Tohoku Medical Megabank Project from MEXT and the Japan Agency for Medical Research and Development (AMED) (Grant Numbers JP20km0105001 and JP21tm0124005). This research used a supercomputer system provided by the Tohoku Medical Megabank Project (funded by AMED under Grant Number JP21tm0424601).
- [1] National Police Agency of Japan Emergency Disaster Countermeasures Headquarters, “Police Countermeasures and Damage Situation associated with 2011 Tohoku district - off the Pacific Ocean Earthquake,” March 10, 2021. https://www.npa.go.jp/news/other/earthquake2011/pdf/higaijokyo_e.pdf [Accessed September 3, 2024]
- [2] R. Kimura et al., “Current status and issues of life recovery process three years after the Great East Japan earthquake questionnaire based on subjective estimate of victims using life recovery calendar method,” J. Disaster Res., Vol.9, No.sp, pp. 673-689, 2014. https://doi.org/10.20965/jdr.2014.p0673
- [3] K. M. Keyes, M. L. Hatzenbuehler, and D. S. Hasin, “Stressful life experiences, alcohol consumption, and alcohol use disorders: The epidemiologic evidence for four main types of stressors,” Psychopharmacol. (Berl)., Vol.218, No.1, pp. 1-17, 2011. https://doi.org/10.1007/s00213-011-2236-1
- [4] K. M. Keyes et al., “Stress and alcohol: Epidemiologic evidence,” Alcohol Res., Vol.34, No.4, pp. 391-400, 2012. https://doi.org/10.35946/arcr.v34.4.03
- [5] F. Gohardehi, H. Seyedin, and S. Moslehi, “Prevalence rate of diabetes and hypertension in disaster-exposed populations: A systematic review and meta-analysis,” Ethiop. J. Health Sci., Vol.30, No.3, pp. 439-48, 2020. https://doi.org/10.4314/ejhs.v30i3.15
- [6] S. Takahashi et al., “Weight gain in survivors living in temporary housing in the tsunami-stricken area during the recovery phase following the Great East Japan Earthquake and Tsunami,” PLOS One, Vol.11, Article No.e0166817, 2016. https://doi.org/10.1371/journal.pone.0166817
- [7] S. Takahashi et al., “Increase in body weight following residential displacement: 5-year follow-up after the 2011 great East Japan earthquake and Tsunami,” J. Epidemiol., Vol.31, Issue 5, pp. 328-334, 2021. https://doi.org/10.2188/jea.JE20190333
- [8] H. Satoh et al., “Evacuation after the Fukushima Daiichi nuclear power plant accident is a cause of diabetes: Results from the Fukushima health management survey,” J. Diabetes Res., Vol.2015, Article No.627390, 2015. https://doi.org/10.1155/2015/627390
- [9] A. Murakami et al., “Association between housing type and gamma γ-GTP increase after the Great East Japan Earthquake,” Soc. Sci. Med., Vol.189, pp. 76-85, 2017. https://doi.org/10.1016/j.socscimed.2017.07.020
- [10] A. Takahashi et al., “Effect of evacuation on liver function after the Fukushima Daiichi Nuclear Power Plant accident: The Fukushima Health Management Survey,” J. Epidemiol., Vol.27, Issue 4, pp. 180-5, 2017. https://doi.org/10.1016/j.je.2016.05.006
- [11] J. A. Fallowfield, M. Jimenez-Ramos, and A. Robertson, “Emerging synthetic drugs for the treatment of liver cirrhosis,” Expert Opin. Emerg. Drugs., Vol.26, Issue 3, pp. 149-163, 2021. https://doi.org/10.1080/14728214.2021.1918099
- [12] K. M. Conigrave et al., “Traditional markers of excessive alcohol use,” Addiction, Vol.98, pp. 31-43, 2003. https://doi.org/10.1046/j.1359-6357.2003.00581.x
- [13] G. M. Lam and S. Mobarhan, “Central obesity and elevated liver enzymes,” Nutr. Rev., Vol.62, No.10, pp. 394-399, 2004. https://doi.org/10.1111/j.1753-4887.2004.tb00010.x
- [14] S. Stranges et al., “Body fat distribution, relative weight, and liver enzyme levels: A population-based study,” Hepatology, Vol.39, No.3, pp. 754-63, 2004. https://doi.org/10.1002/hep.20149
- [15] A. Fraser et al., “Alanine aminotransferase, gamma-glutamyltransferase, and incident diabetes: the British Women’s Heart and Health Study and meta-analysis,” Diabetes Care., Vol.32, No.4, pp. 741-50, 2009. https://doi.org/10.2337/dc08-1870
- [16] N. Ghouri, D. Preiss, and N. Sattar, “Liver enzymes, nonalcoholic fatty liver disease, and incident cardiovascular disease: A narrative review and clinical perspective of prospective data,” Hepatology, Vol.52, No.3, pp. 1156-61, 2010. https://doi.org/10.1002/hep.23789
- [17] E. Hemmingsson, “A new model of the role of psychological and emotional distress in promoting obesity: Conceptual review with implications for treatment and prevention,” Obes. Rev., Vol.15, No.9, pp. 769-79, 2014. https://doi.org/10.1111/obr.12197
- [18] L. Darwish et al., “Depression in people with type 2 diabetes: current perspectives,” Diabetes. Metab. Syndr. Obes., Vol.11, pp. 333-43, 2018. https://doi.org/10.2147/dmso.s106797
- [19] K. Spiegel et al., “Sleep loss: A novel risk factor for insulin resistance and type 2 diabetes,” J. Appl. Physiol., Vol.99, Issue 5, pp. 2008-2019, 2005. https://doi.org/10.1152/japplphysiol.00660.2005
- [20] K. Spiegel et al., “Effects of poor and short sleep on glucose metabolism and obesity risk,” Nat. Rev. Endocrinol., Vol.5, pp. 253-61, 2009. https://doi.org/10.1038/nrendo.2009.23
- [21] D. E. R. Warburton, C. W. Nicol, and S. S. D. Bredin, “Health benefits of physical activity: The evidence,” CMAJ, Vol.174, No.6, pp. 801-809, 2006. https://doi.org/10.1503/cmaj.051351
- [22] M. C. Venables and A. E. Jeukendrup, “Physical inactivity and obesity: links with insulin resistance and type 2 diabetes mellitus,” Diabetes Metab. Res. Rev., Vol.25, pp. S18-S23, 2009. https://doi.org/10.1002/dmrr.983
- [23] K. Ito et al., “Housing type after the Great East Japan Earthquake and loss of motor function in elderly victims: A prospective observational study,” BMJ Open, Vol.6, Issue 11, Article No.e012760, 2016. https://doi.org/10.1136/bmjopen-2016-012760
- [24] T. Sone et al., “Longitudinal association between time-varying social isolation and psychological distress after the Great East Japan Earthquake,” Soc. Sci. Med., Vol.152, pp. 96-101, 2016. https://doi.org/10.1016/j.socscimed.2016.01.037
- [25] Y. Sasaki et al., “Does type of residential housing matter for depressive symptoms in the aftermath of a disaster? Insights from the great East Japan earthquake and tsunami,” Am. J. Epidemiol., Vol.187, Issue 3, pp. 455-64, 2018. https://doi.org/10.1093/aje/kwx274
- [26] A. Hozawa et al., “Study profile of the Tohoku medical Megabank community-based cohort study,” J. Epidemiol., Vol.31, Issue 1, pp. 65-76, 2021. https://doi.org/10.2188/jea.je20190271
- [27] N. Nakaya et al., “Degree of housing damage caused by the Great East Japan Earthquake and all-cause mortality in the community-based cohort study of the Tohoku Medical Megabank Project,” J. Epidemiol. Community Health, Vol.79, Issue 6, pp. 451-458, 2025. https://doi.org/10.1136/jech-2024-223084
- [28] R. C. Kessler et al., “Short screening scales to monitor population prevalences and trends in non-specific psychological distress,” Psychol. Med., Vol.32, Issue 6, pp. 959-976, 2002. https://doi.org/10.1017/s0033291702006074
- [29] C. R. Soldatos, D. G. Dikeos, and T. J. Paparrigopoulos, “Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria,” J. Psychosom. Res., Vol.48, Issue 6, pp. 555-560, 2000. https://doi.org/10.1016/s0022-3999(00)00095-7
- [30] R. Kimura, “Support that disaster victims of the 2011 Great East Japan Earthquake felt and considerations on how to formulate measures for disaster management in the future—Based on a comparison with the 1995 Great Hanshin Awaji (Kobe) earthquake, the 2004 Mid-Niigata Earthquake and the 2007 Chuetsu-Oki Earthquake,” J. Disaster Res., Vol.17, Issue 2, pp. 183-196, 2022. https://doi.org/10.20965/jdr.2022.p0183
- [31] A. M. Al-khaykanee, A. G. Hamad, and S. A. Hussein, “A review about liver function tests,” GSC Biol. Pharm. Sci., Vol.30, No.1, pp. 213-217, 2025.https://doi.org/10.30574/gscbps.2025.30.1.0023
- [32] A. Unalp-Arida and C. E. Ruhl, “Noninvasive fatty liver markers predict liver disease mortality in the U.S. population,” Hepatology, Vol.63, No.4, pp. 1170-1183, 2016. https://doi.org/10.1002/hep.28390
- [33] P. Ke et al., “Association of the serum transaminase with mortality among the US elderly population,” J. Gastroenterol. Hepatol., Vol.37, Issue 5, pp. 946-953, 2022. https://doi.org/10.1111/jgh.15815
- [34] S. K. Kunutsor, T. A. Apekey, and H. Khan, “Liver enzymes and risk of cardiovascular disease in the general population: A meta-analysis of prospective cohort studies,” Atherosclerosis, Vol.236, Issue 1, pp. 7-17, 2014. https://doi.org/10.1016/j.atherosclerosis.2014.06.006
- [35] G. Koenig and S. Seneff, “Gamma-glutamyltransferase: A predictive biomarker of cellular antioxidant inadequacy and disease risk,” Dis. Markers., Vol.2015, Article No.818570, 2015. https://doi.org/10.1155/2015/818570
- [36] T. H. Lee et al., “Serum aminotransferase activity and mortality risk in a United States community,” Hepatology, Vol.47, No.3, pp. 880-887, 2008. https://doi.org/10.1002/hep.22090
- [37] Miyagi Prefectural Government, “Recovery of Miyagi in numbers.” https://www.pref.miyagi.jp/documents/900/742408.pdf [Accessed September 5, 2024]
- [38] Miyagi Prefectural Government, “Health survey for residents of emergency temporary housing (prefab units and privately leased rental housing),” 2023 (in Japanese). http://www.pref.miyagi.jp/soshiki/kensui/oukyuukasetsujyutaku.html [Accesed January 15, 2024]
This article is published under a Creative Commons Attribution-NoDerivatives 4.0 Internationa License.